AKI in Cirrhosis
Renal dysfunction is a common complication in hospitalized patients with cirrhosis. The diagnosis of Type 1 Hepatorenal syndrome (HRS) is one of exclusion and cannot be made until other causes of renal failure, particularly acute tubular necrosis (ATN), are ruled out. The treatment for ATN is solely supportive via hemodialysis. Differentiating between Type 1 HRS and ATN may be difficult and often takes several days, as traditionally-used distinguishing common urinary parameters may be altered in advanced liver disease. Additionally, it is challenging to differentiate patients who are at risk for AKI progression early in the course of their disease. Crucial delays in diagnosis impair the ability to begin early treatment which can lead to increased morbidity and mortality. Research in both experimental animals and humans has identified urine biomarkers that are capable of detecting renal tubular injury, a prerequisite for ATN with high degrees of sensitivity and specificity which also associate with AKI progression. In this prospective multicenter cohort study, we enrolled ~200 patients from four major academic medical centers with cirrhosis and renal dysfunction. Our mission is twofold – (1) to determine the ability of urinary IL-18, NGAL, KIM-1, and L-FABP to correctly differentiate between Type 1 HRS and ATN and (2) to evaluate the association of these biomarkers with AKI progression and mortality to identify high risk patients.
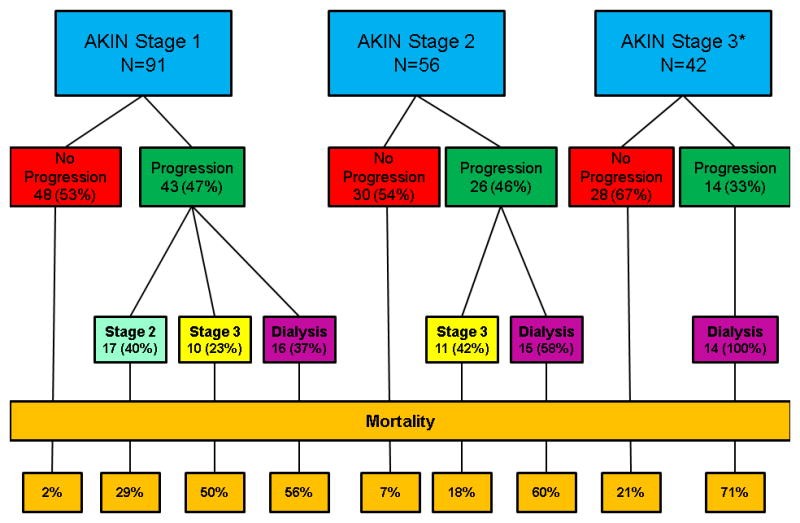
Belcher JM, Garcia-Tsao G, Sanyal AJ, Bhogal H, Lim JK, Ansari N, Coca SG, Parikh CR; TRIBE-AKI Consortium. Association of AKI with mortality and complications in hospitalized patients with cirrhosis. Hepatology 2013; 57(2):753-62.
Funding Information for this Project
This study was supported by the NIH/NIDDK (1R21-DK078714, “Identifying Acute Tubular Necrosis in Cirrhosis Patients with Renal Dysfunction”)